
Low Back Pain Info - Part 1
SOME GENERAL GUIDELINES FOR BACK PAIN
Back Pain can be undaunting - no doubt about it!
If you suffer with back pain, you probably already know there is no one way or even any standard way for that matter, to fix it. Strep infections have penicillin. There is no “penicillin” for back pain. Finding a clinician who can help relieve some of your symptoms is certainly a trial itself. Many, if not most of us, have been there.
In Part, I will provide some standard and recognized guidelines from the medical community to know and think about if you suffer from back pain.
In Part 2, I will provide some of my thoughts and opinions from my many, many years of experience in treating back pain symptoms (including my own,) and from changing my approach to treating back pain umpteen times.
1. GENERAL PRACTICAL PRACTICE GUIDELINES FORLOW BACK PAIN
While there are many things that clinicians and physicians disagree about in the care of back pain, here is the somewhat official list of what is agreed upon for back pain in the medical community:
· Rule out specific spinal pathology or other pathology that can cause back pain
· No routine use of imaging for non-specific pain - (see #2 below for more info on imaging guidelines and reasoning behind it.)
· High quality patient education – including pain science education
· Physical Exercise – Movement or activity should be based on patient preference or what patient will actually do. Active motion is better than passive.
· Manual Therapy (manipulation, mobilization, massage) combined with exercise is best, better than exercise alone.
· Early return to activity
· Caution with Opioids
· Promote Self-Management - (Freda agrees strongly with this one, once what works for your pain is figured out.)
· Assess and manage psychosocial factors – refer for psychological or cognitive therapy when indicated
2. IMAGING
WHEN IMAGING IS NOT RECOMMENDED
In the absence of red flags, imaging is no longer recommended for:
· Acute pain within the first 30-45 days - (“Imaging for low back pain in the first six weeks after pain begins should be avoided in the absence of specific clinical indications (e.g., history of cancer with potential metastases, known aortic aneurysm, progressive neurological deficit, etc.). Most low back pain does not need imaging and doing so may reveal incidental findings that divert attention and increase the risk of having unhelpful surgery.”) American Society of Anesthesiologists – Pain Medicine January 21, 2014. * SEE CHART BELOW *
· Low back pain with referred pain (as in some hip or butt pain) especially in people over age 65. (Referred pain often increases with walking and decreases with rest.)
· Chronic low back pain related to generalized pain
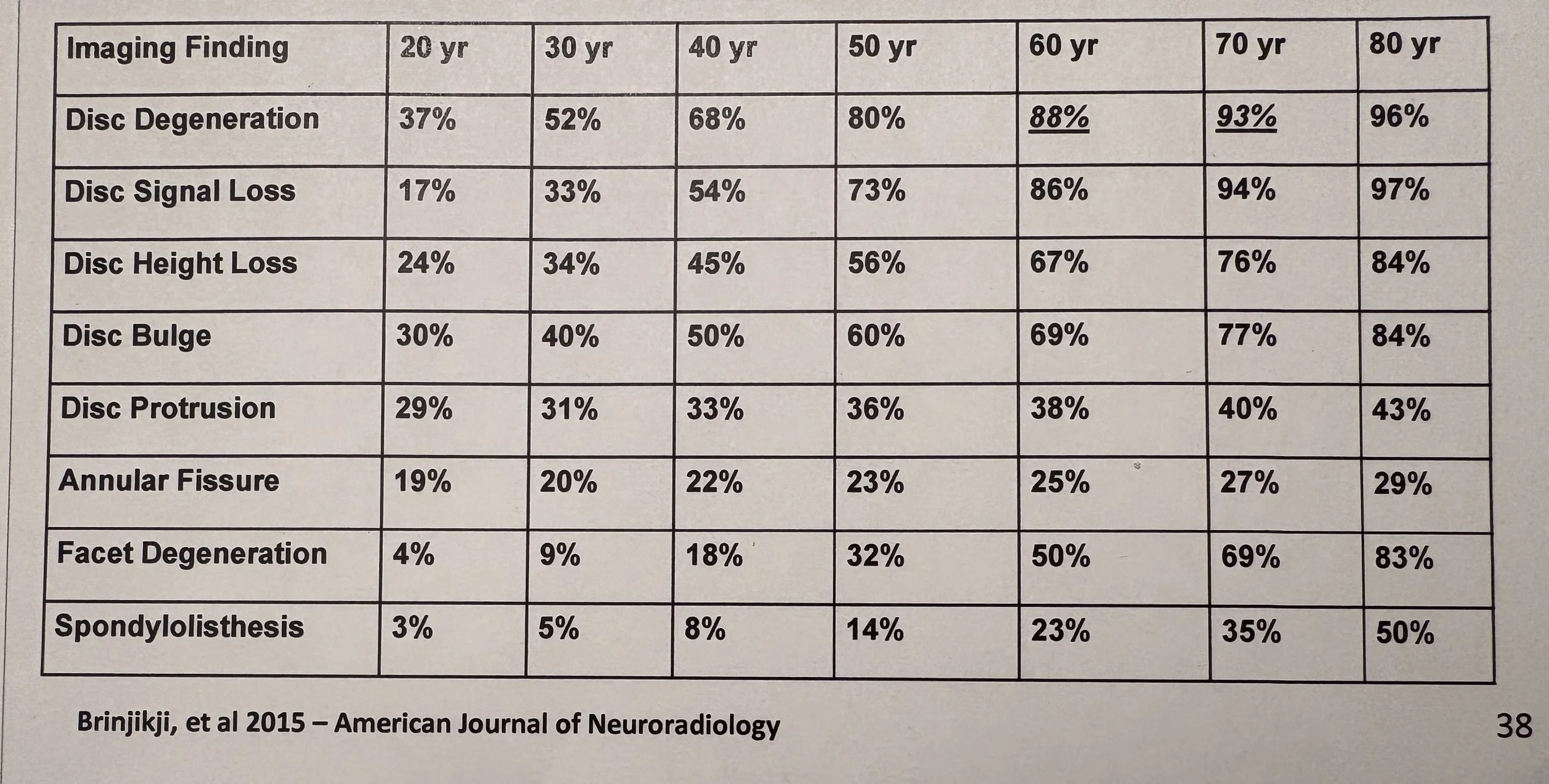
CHART *
The following chart shows image findings in people who have NO back pain. Various degrees of spinal degeneration are present in high proportion without symptoms. Thus, what might be found in imaging may not be causing the problem and can divert attention away from the problem or increase a patient’s anxiety about their back pain.
WHEN IMAGING IS RECOMMENDED
Imaging is recommended for:
· Low back pain with radiating pain
· In progressive neurological conditions
· When surgery ss potentially indicated
· When one is a candidate for epidural injections
· With other clinical findings such as central canal stenosis with bowel and bladder changes, root compression with muscle weakness that does not change with movement or position changes
3. ACUTE PAIN vs CHRONIC PAIN
Back pain is considered to be acute if you have had pain for 3 months or less.
Back pain is considered chronic if it has occurred for 3 months or more. Chronic pain may be more associated with other generalized pain or psychosocial issues.
Intermittent, “on and off” pain is not particularly noted in the literature, but Freda has seen this a lot and will address in part 2.
STAY TUNED FOR PART 2 WHERE TOPICS WILL INCLUDE INFO ON EXAMINATION, TREATMENT AND FREDA’S THOUGHTS ON LOW BACK PAIN THROUGH EXPERIENCE